Dr. Chris Winfree Treats Parsonage-Turner Syndrome with a Phrenic Nerve Hourglass Constriction
An Innovative Approach to Regain Function via Peripheral Nerve Surgery

Dr. Chris Winfree, Director, Center for Peripheral Nerve Surgery has treated neuralgic amyotrophy (an autoimmune disorder in which the body's immune system produces antibodies that attack the peripheral nerves) for decades. In unique cases of Parsonage-Turner Syndrome, there are special considerations as this diagnosis can cause structural abnormalities in the affected peripheral nerves that can prohibit a patient's recovery. A phrenic nerve injury can occur anywhere along its course and clinically results in diaphragm paralysis. Although most patients with Parsonage-Turner syndrome and phrenic nerve dysfunction improve without treatment, some patients do not recover spontaneously. In these cases, an initial autoimmune response produces scarring along the affected nerve(s). This scar, known as an hourglass constriction, causes focal compression of the nerve at the scar's site, preventing the nerve from spontaneously recovering. This case shows a unique example of phrenic nerve injury secondary to Parsonage-Turner syndrome that improved with internal neurolysis.
This surgical case features a 64-year-old male with a remote history of a fall who is neurologically intact. Two weeks later, he developed exertional shortness of breath. The initial workup demonstrated a chest x-ray showing an elevated right hemidiaphragm. A right phrenic nerve pathology was suspected. The patient presented with delayed diaphragmatic paralysis. No obvious injury mechanism is evident, and this pattern is consistent with a painless variant of Parsonage-Turner syndrome. Most patients with phrenic nerve involvement improve with conservative treatment; however, some patients do not recover spontaneously. The initial autoimmune response produces scarring along the affected nerves in these cases. This scar, called an hourglass constriction, is a well-described pathological finding in Parsonage-Turner syndrome and causes focal compression and also thought to be a reason why a subset of Parsonage-Turner patients do not make a full recovery.
Dr. Winfree says, "We investigated the possibility that an hourglass constriction could be present and obtained high-resolution phrenic nerve imaging and eventually obtained a high-resolution ultrasound, which showed the hourglass constriction." With the diagnosis of Parsonage-Turner syndrome confirmed, Dr. Winfree says, "The decision to surgically decompress the hourglass constriction was made, given the fact that we were still within one year from the symptoms to allow for reinnervation, the process of restoring nerve function to a previously denervated (lost nerve supply) area of the body.”
Click here to access the full surgical video via The JNS Neurosurgical Focus Video.
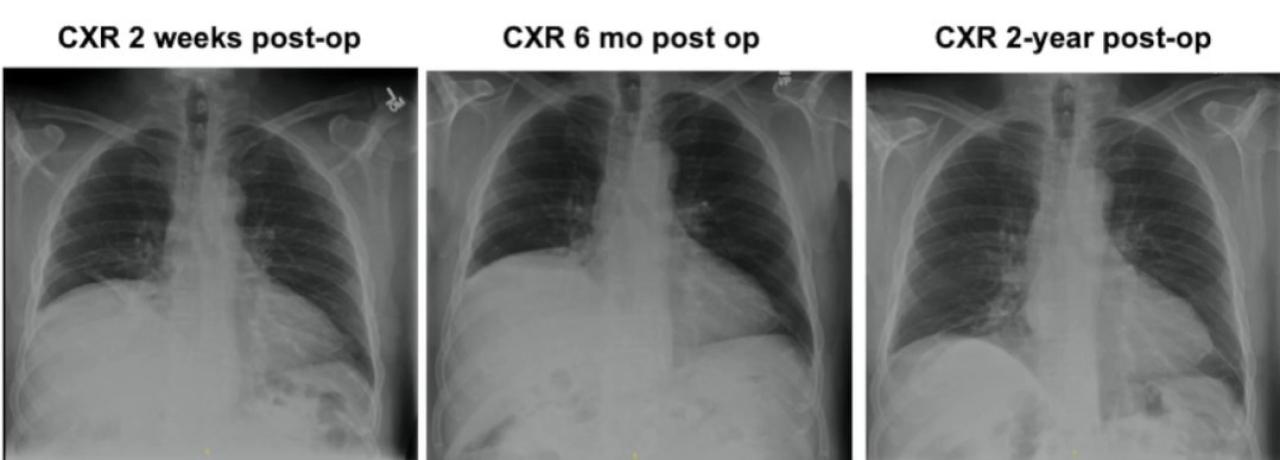
Following the surgery, the initial 2-week follow-up chest x-ray showed no change from baseline. The 6-month follow-up also showed no change from baseline. However, the 2-year follow-up chest x-ray showed the resolution of the patient's elevated hemidiaphragm. Additionally, the patient's exertional dyspnea was resolved by the 2-year follow-up visit. Dr. Winfree shares, "This was our first patient with Parsonage-Turner syndrome with hourglass constriction that we treated in our Diaphragm Paralysis Center. We look forward to reporting on additional patients as 2-year follow-up data becomes available.
Dr. Winfree shares, "This was our first patient with Parsonage-Turner syndrome with hourglass constriction that we treated in our Diaphragm Paralysis Center. We have treated several additional patients and look forward to reporting on their 2-year follow-up data as it becomes available.”
